Fagfellevurdert

Norwegian Psychomotor Physiotherapy: A scoping review
Vitenskapelig artikkel
Tove Dragesund, fysioterapeut PhD, førsteamanuensis. Fakultet for Helse- og Sosialvitskap, Høgskulen på Vestlandet. tove.dragesund@hvl.no.
Aud Marie Øien, fysioterapeut PhD, førsteamanuensis. Fakultet for Helse- og Sosialvitskap, Høgskulen på Vestlandet.
Denne vitenskapelige artikkelen er fagfellevurdert etter Fysioterapeutens retningslinjer, og ble akseptert 5.desember 2022. Ingen interessekonflikter oppgitt.
Abstract
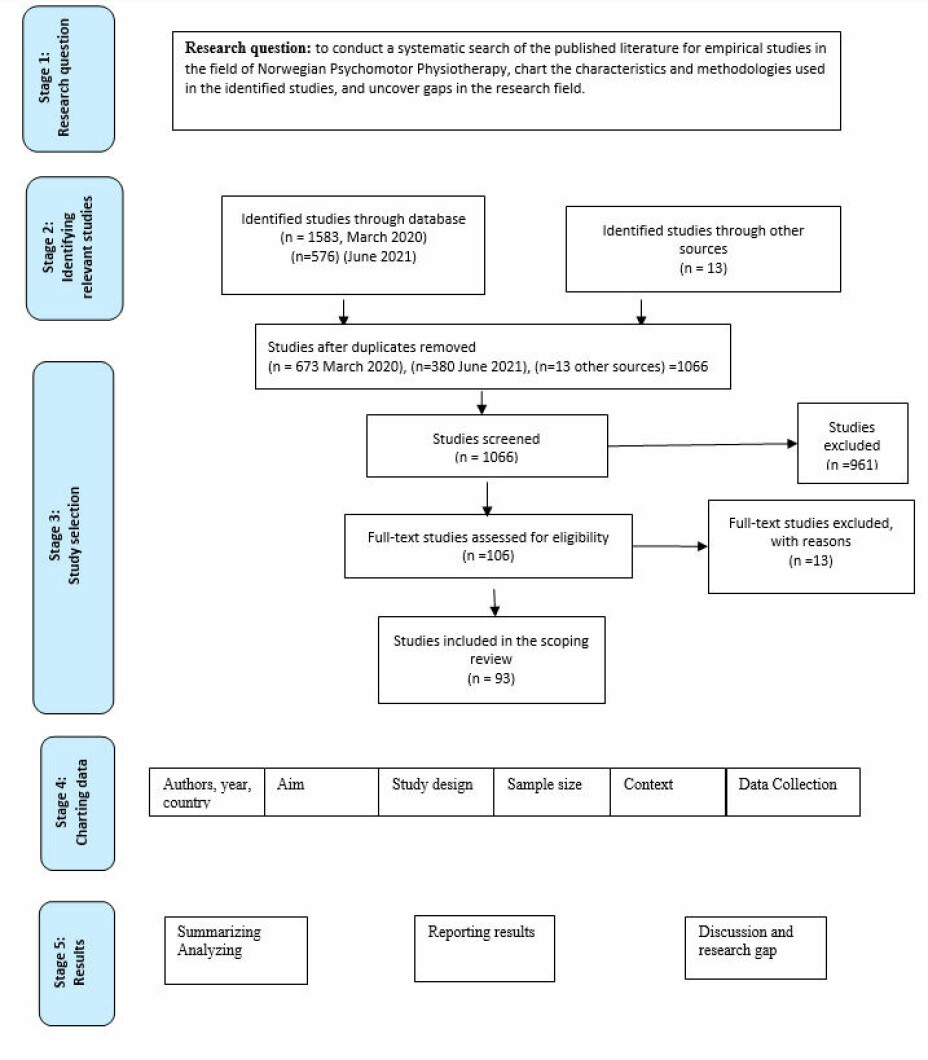
Background: Norwegian Psychomotor Physiotherapy (NPMP) is an established treatment approach mainly applied to patients with long-lasting musculoskeletal pain. The research in the field of NPMP is gradually expanding. The aim of this study was therefore to conduct a systematic search of the published literature for empirical studies in the field, to chart the characteristics and methodologies used and uncover gaps in the research field.
Methods: A scoping review methodology was chosen.
Results: A total of 93 full text research articles were analysed. The analysis identified primarily articles with a quantitative approach concerning development and standardisation of the NPMP body examination into scales. The qualitative studies concerned different experiences from the body examination and the treatment approach from the patients’ and/or the physiotherapists’ perspectives.
Conclusion: The literature in the field is limited but has slowly expanded during the last 20 years. More research is generally needed to further develop and expand the treatment approach.
Keywords: Norwegian Psychomotor Physiotherapy, Scoping review, Quantitative methods, Qualitative methods
Norsk psykomotorisk fysioterapi. En scoping review studie
Sammendrag
Hensikt: Norsk psykomotorisk fysioterapi (NPMF) er en etablert behandling tilnærming primært for pasienter med langvarige muskel- og skjelett smerter og sammensatte lidelser. Forskning innen fagfeltet er i utvikling. Hensikten med denne studien var derfor å gjennomføre et systematisk søk av den publiserte litteraturen i fagfeltet for å kartlegge omfang, metodisk tilnærming og å bidra til å avdekke kunnskapshull.
Metode: Scoping review ble valgt som metode.
Resultater: I alt ble 93 artikler analysert. Analysen avdekket primært artikler med en kvantitativ tilnærming som omhandlet utvikling og standardisering av kroppsundersøkelsen i NPMF. De kvalitative studiene omhandlet ulike erfaringer fra kroppsundersøkelsen og behandlingstilnærmingen fra pasientenes og eller fysioterapeutenes perspektiv.
Konklusjon: Litteraturen i fagfeltet er begrenset, men har gradvis ekspandert de siste 20 årene. Mer forskning er generelt nødvendig for å videreutvikle behandlingstilnærmingen.
Nøkkelord: Norsk psykomotorisk fysioterapi, Scoping review, Kvantitative metoder, Kvalitative metoder.
Introduction
Long-lasting musculoskeletal pain is characterized by reduced physical function, often linked with anxiety and depression, and with increased risk of developing other health conditions, early retirement, reduced wealth, and social participation, and increased all-cause mortality (1).
Norwegian Psychomotor Physiotherapy (NPMP) is a physiotherapeutic approach applied to patients with long-lasting musculoskeletal pain and complex health complaints (2, 3). The approach emerged from the collaboration between the physiotherapist Aadel Bülow-Hansen and the psychiatrist Trygve Braatøy (1946-1951) (2, 3). Bülow-Hansen and Braatøy collaborated by treating the same patients and discussing experiences and theories. One major interest during their collaboration was how muscular tension, breathing and emotions interdepended and mutually influenced each other(2, 3). As such their approach conceptualized the reciprocal relationship between restrictions and regulations of muscular tension, breathing, movements and emotions (2,3).
Since 1952, the treatment approach has furthered developed being a specialization in physiotherapy. From 1994 the education was a post graduate education at Oslo University College of Applied Sciences, and from 2000 at the Artic University of Norway, Tromsø (UiT) (2). Further, the education was at a level of master’s degree at UiT since 2010, at the Western Norway University of Applied Sciences and the Oslo Metropolitan University since 2018 and 2021, respectively.
The research in the field of NPMP is gradually expanding. Hence a review might provide an overview and bring together the research in the field (6). The aim was therefore to 1) conduct a systematic search of the published literature of empirical studies in the field of NPMP, 2) chart the characteristics and methodologies used in the identified studies, 3) and uncover gaps in the research field.
Methods
A scoping review methodology is well suited for mapping the size and scope of research on a topic, synthesizing findings, and identifying gaps in the literature (4). The approach is further appropriated given the expectation of finding papers with diverse methodology (4). We followed the framework for scoping reviews originally described by Arksey and O’Malley (5) and later advanced by Levac et al. (6) and Khalil et al. (7).
Identifying relevant studies
Relevant peer-reviewed articles were identified in the databases: The Cochrane Library, Epistemonikos, PEDro (The Physiotherapy Evidence Database), AMED, Cinahl, Scopus, Medline, Embase, Forskningsdatabasen.dk, Norart, Oria, Web of Science, SveMed+, Idunn, Google Scholar. The searches were conducted in March 2020 and in June 2021. The search terms used to identify the relevant studies were psychomotor physiotherapy, psychomotor physical therapy, Psykomotorisk fysioterapi [psychomotor] AND [physiotherapy] (appendix).
No restrictions were placed on the study search to ensure inclusion of the full breadth of the literature.
Study selection
To
capture the breadth of the literature, articles were included if it: 1) was
peer-reviewed, 2) contained NPMP treatment and or elements from the treatment
approach, 3) contained the body-examination in NPMP or elements of the
examination. No limitation was set for year of publication. Articles were
excluded if they: 1) were not peer-reviewed, 2) not written in English or
Scandinavian languages.
After the identification of the citations in the electronic database search, the first screening focused on the title and abstract (n=1066). Following this, the authors independently screened the possible articles to be included in the further analysis. A total of 106 articles were chosen to be studied further (Figure 1). The authors then considered these articles and excluded 13 articles because they were not peer-reviewed. Finally, this process ended in including 93 articles (Figure 1).
Charting extraction
Information about the studies is described in table 1.
Data synthesis and analysis
The studies were further analysed to gain insight into the results presented in the studies. During this process, the identified studies were re-read to further extract the results. The methodology and perspectives in the studies varied. Consequently, we divided the studies in three groups: quantitative studies, qualitative studies, and studies including both qualitative and quantitative methods. The quantitative studies were thematic divided in, patients receiving NPMP, examination and outcome of the treatment. The qualitative studies were divided in empirical studies from the patients’ and the physiotherapists’ perspectives, and theoretical articles.
Results
Distribution of publications and methodology
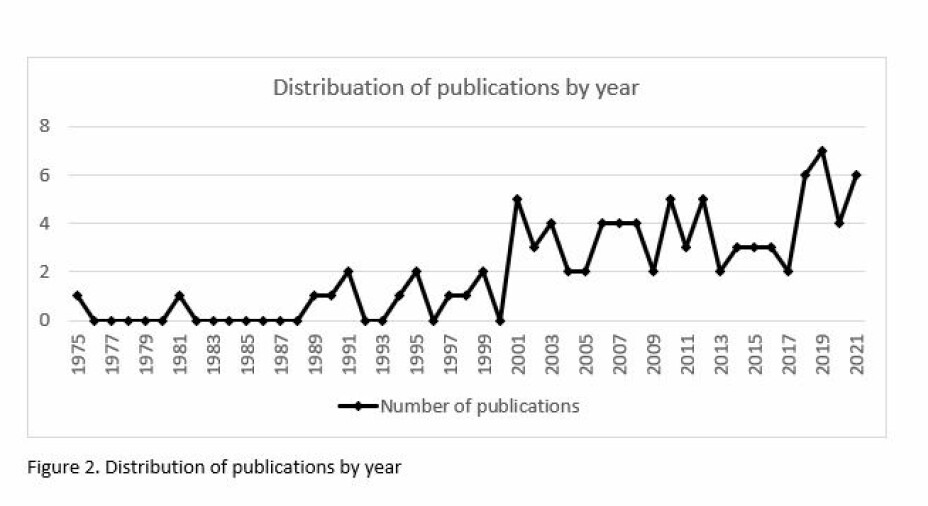
The included 93 full text articles were from 1975 to 2021 and most of them were conducted in Norway (n=87) (Figure. 1, Table 1). Eighteen of the years had no publications, twenty-one of the years had either one, two or three publications and the years 2001, 2003, 2006, 2007, 2008, 2010, 2012, 2014, 2018, 2019, 2020 and 2021 had 4 or more publications (Figure 2).
A total of 68 studies were written in English and published in international journals. Most of the studies used quantitative approaches (n=51). Among these studies, 21 concerned development and evaluation of psychometric properties of different test scales emerged from the NPMP body examination (8-28). Three studies included development and evaluation of a body awareness questionnaire (29-31). There were five outcome studies of NPMP treatment, including three randomized controlled studies (RCT)(32-36). Among the other quantitative studies, 20 included the use of one of the scales, emerged from the NPMP body examination or elements from the NPMP treatment approach (36,39-57).
One study included both a quantitative and a qualitative approach (58).
Among the qualitative studies, 15 studies (59-73) explored experiences from the physiotherapist’s perspective, 10 studies (74-83) from the patients’ perspectives and three studies (84-86) from both the physiotherapist and the patients’ perspectives. There were two case studies (87, 88) and seven theoretical studies (89-95). The theoretical perspectives in the qualitative studies were, in addition to NPMP, primarily Merleau-Ponty’s phenomenology of perception. However, different perspectives for example from social science, psychology and communication theories were also used.
The sample size in the studies varied from 1-416 participants, mainly being patients with musculoskeletal pain or mental health problems. The physiotherapists were specialized in NPMP. Most of the studies were conducted in primary health care or mental health clinics.
Quantitative studies
Patients receiving NPMF
Characteristics of the patients referred to NPMP treatment were described in two studies (32,96). The patients (80-82%) were primarily women, with a mean aged at 42 years. Their main symptoms were long-lasting, local, or general musculoskeletal pain and tension. Two third of the sample presented mixed symptoms, mainly with depression, anxiety, and musculoskeletal pain.
Examination
Based on the body examination of NPMP, a clinical examination tool was developed (89) to evaluate short-term dynamic psychotherapy (37). The findings indicated that 53.3 % of the patients improved on the scores on the body examination tool. A positive change on the scores were also strongly correlated with psychological improvement. A similar examination tool was used to examine dental, psychological and bodily ailments in a group of female patients with myofascial pain-dysfunction. The examination revealed that the patients had increased muscular tension and an inadequate respiratory function (38).
Furthermore, two different, test scales: the Global Physiotherapy Examination-52 (GPE-52) and the Comprehensive Body Examination (CBE) are developed. The GPE-52 is developed from Sundsvold’s (8, 9) assessment method, and further psychometric evaluated (13, 14, 18-20, 22). The scale includes 52 single tests distributed in the 5 body domains; body posture, respiration, movement, muscle, and skin quality and was found to be reliable and valid for assessing localisation and degree of physical aberrations in patients with long-lasting musculoskeletal pain. The CBE are based on the clinical body examination called Resource Oriented Body Examination (ROBE) and further developed and evaluated in several studies (10-12, 15-17). The CBE also revealed physical aberration in the 5 body domains described above. Later, the two scales, GPE-52 and CBE, are further merged into one scale: the Global Body Examination (GBE) (23-28).
The ROBE is also merged into a shorter scale, the ROBE II, that distinguished bodily characteristics between patients with psychosomatic, musculoskeletal, and schizophrenic disorders (21).
A self-reported questionnaire reflecting the phenomenon of body awareness; the Body Awareness Rating Questionnaire (BARQ) is developed for evaluative purposes (29, 30) and further revised (35). The revised BARQ-R being a unidimensional and feasible measurement for assessing the phenomenon of body awareness in the context of body-mind approaches for patients with musculoskeletal pain problems (31).
The scales of the ROBE (39), the ROBE II (42, 43), the GPE-52 (36, 42, 44, 48, 49, 55,57), the CBE (40,41) and the GBE (50), are used to assess and characterise body ailments of participants in different studies or to evaluate the outcome of a treatment (36,46, 47).
Outcome
Outcomes of NPMP treatment are evaluated in two different one-group studies (32, 46) and one study with a compared group on a waiting-list (33). The studies showed that NPMP has the potential for reducing symptoms like health complaints, depression, anxiety, insomnia, fatigue and improving quality of life.
One randomized controlled study of long-term NPMP in groups, indicated additional improvement of symptoms and a higher rate of return to work (34).
Two studies evaluated individual NPMP treatment, one with a control group on waiting-list (35) and another with a control group receiving Cognitive Patient Education combined with active individualized physiotherapy (COPE-PT) (36, 49). The results from the first study showed that 6-month NPMP increased the patients’ experiences of quality of life and self-esteem, and reduced pain. The second study showed that NPMP contributed to improve pain and physical function. However, COPE-PT, targeted towards pain-coping and increasing activity, contributed to somewhat more improvements on some of the outcome measures than NPMP at 6- and 12-month follow-up.
Elements from NPMP approach are also included in different studies including patients suffering from dizziness (54), chronic pain (51) and patients with migration experiences (53, 56).
Qualitative studies
Patients’ perspective
Studies from the patients’ perspectives included experiences of the NPMP examination (74), and experiences of NPMP massage (75) and of breathing (78,79) after completed NPMP treatment. The body examination had a great impact on the patients’ understanding of their own ailments. The NPMP massage enhanced relaxation as well as perception and reflection on own body, while experiences of breathing enabled the patients to better understand the interaction between breathing and well-being.
The patients’ embodied experiences of change after NPMP treatment are described to enhance self-perception and self-knowledge. Examples like; being more in touch with and familiar with their body and self, to be better acquainted with bodily reactions and to better interpret bodily symptoms and to connect these reactions to relational dimensions and habitual ways of acting. The relation to and the interaction (verbal and nonverbal) with the physiotherapists during the treatment seemed crucial. The patients valued the physiotherapists’ sensitivity, their ability to be trusted and adjust the treatment to their needs. They also appreciated to be given enough time and space to explore how to become more in contact with their bodies. The experiences described above seemed to be prerequisites for the patients’ changing process during the treatment (75- 83, 85, 87).
Action research aiming to improving professional practice for counsellors in social work are studied (98, 99) emphasizing that the supervision based on NPMP movements, opened access to personal learning and contributed to increased self-knowledge in professional social work practices.
The patients’ experiences from a self-management intervention program including principles and element from NPMP treatment are also explored (52).
Physiotherapists’ perspective
From the physiotherapists’ perspective, the implicit verbal and non-verbal communication during the NPMP examination are studied (59, 60), as well as the physiotherapists’ clinical reasoning process during the examination (61-64,100). The studies showed how practice, and way of thinking could differ among the physiotherapists in different clinical contexts; a NPMP therapist, a manual therapist, and a district physiotherapist. The relationship, context, and actual basis of cooperation were influenced by how the physiotherapists related to the patients’ bodies.
The physiotherapists‘ experiences from demanding treatment processes (68) and the impact of own embodied knowledge in clinical practice (69) underscored the value of being sensitive and self-aware during the treatment. The physiotherapists searched to adjust their therapeutic approaches, depending on the individual patient’s specific problems and degree of emotional and bodily strain. They experienced the importance of creating a common ground with the patients, inviting them to involve themselves in the treatment.
In treatment of torture survivors and patients with adverse child abuse, the physiotherapists experienced that tailoring both the examination and the treatment to the individual patient were crucial (67, 88). In an outpatient clinic for mental health, the bodily approach in NPMP seemed to contribute with something different from and complementary to the verbally approaches in the interdisciplinary team treating patients with eating disorders (66). The physiotherapists experienced that the use of touch in treatment of patients with anorexia neurosis were challenging. However, being aware of and adjust the touch to the patient’s bodily reactions contributed to give the patients comfort and security (73).
The professional development in the field of NPMP was described as a gradual process, integrating theory and experiences from practice. Clinical experiences and contact with colleagues were the most significant sources of development (65). Reflections about the approach from the perspective of highly experienced NPMP physiotherapists concluded that a complex understanding of body knowledge to meet each patient's compound problems is needed (70).
The closing down during the Covid-19 pandemic impacted the practicing of NPMP (72). The approach was performed in new ways, illuminating how video-consultation in contrast to hands - on, could be offered to the patients.
The communication process during long-term treatment, explored from both the patients’ and the physiotherapists’ perspective, emphasised that demanding episodes generated a potential for development and improvement of the treatment outcomes. Understanding such episodes as open and dynamic, in contrast to defining the patient as demanding, suggested to be a useful perspective during the treatment (84, 86).
Experiences from a long-term collaboration between a physiotherapist and a psychologist treating the same patients described how reduced body awareness seemed to correspond with fragmented memories of their own life history and how enhanced body awareness became a vital aspect in the therapeutic processes (101).
Theoretical studies
Theoretical aspects of Braatøy’s thinking, underpinning the NPMP treatment, were analysed considering Løgstrup’s philosophy (90-92). The approach was presented as a bodily-existential process (90). Embodied awareness was discussed with the distinction between awareness in the senses and awareness in understanding (9)1. The everyday language rooted in sensation, might have possibilities to overcome the gap between body and mind (92).
A theoretical article concerning anorexia nervosa underscored the value of addressing bodily restraints in the treatment approach (93). Another article describing contribution factors and treatment implications of exercised induced laryngeal obstruction (EILO) in athletes, emphasized the physiotherapist skills and competence regarding examining breathing patterns and postural de-alignments in the treatment process (94).
Exploring a narrative approach to long-term NPMP treatment indicated that emergent narratives point to potential moments of change and seem to be a useful supplement in the treatment (95).
Qualitative and quantitative study
One study focused on evaluating the effect of NPMP treatment on exercise-induced laryngeal obstruction in elite athletes (58). The study underscored how a diaphragmatic breathing pattern, a more balanced tension in respiratory muscles, and sound cervical alignment and stability might help to reduce adverse stress on the respiratory system and optimise the function of the larynx during high-intensity exercise.
Discussion
This scoping review identified an informative number of articles, primarily conducted in Norway and with a quantitative approach concerning development and standardisation of the NPMP body examination into test scales. The qualitative studies concerned different experiences from the body examination and the treatment approach from the patients’ and/or the physiotherapists’ perspectives.
The number of studies concerning development and evaluation of the measurement properties of GPE-52, CBE and GBE were surprising. The scales include examination of the body through 5 body domains. Scores on the different domains are summarized into sub-scores and further into a sum score, reflecting body ailment and resources (10-20,22-28,36,39-50,55,57). Hence the scales seem to have the possibility to reveal in which domain(s) the ailments are localized and how the whole body are functionally influenced by the ailments.
One strength with NPMP is the individually tailoring of the approach according to each patients need (2,3). Using the phenomenological perspective of the body (103), as theoretical perspectives in the included qualitative studies in this review, has contributed to improve the understanding of the phenomenon of long-lasting musculoskeletal pain, as well as the NPMP approach for patients with such pain problems. The patients included in the studies, described their experiences of the verbal and nonverbal interaction with the physiotherapists both during the NPMP examination and treatment. The NPMP examination impacted the patients’ understanding of their own ailments. The patients further described how enough time and space to explore and reflect upon body sensations, new ways of moving and acting during the treatment were valuable. Gradually, they described that the
treatment process increased body contact and made them more aware how history and life influenced their symptoms and ailments with a need to take better care of themselves during daily life (74-83, 84, 86). As such the treatment seem to contribute to an enhanced self-perception and -understanding. Earlier studies have described how patients with long-tasting musculoskeletal pain for years consult specialists for help to make sense of their illness and to confirm the reality of symptoms (104-106). Thus, living with long-lasting musculoskeletal pain is described as a long and lonely struggle for health care (106). As such NPMP seem to meet requires and needs patients with such pain problem might have.
From the physiotherapists’ perspectives, the NPMP treatment of patients with complex health problems, were experienced as challenging with the need to be anchored in themselves and adjust the treatment approach according to the patients’ response. These findings seem to correspond with studies from similar therapeutic settings, where the therapist’s own body awareness, empathy, trust, and acceptance as well as direction and advances in the therapeutic process are emphasized (107-109).
Within treatment of patients with long-lasting and complex health complaints, a dilemma still exists between experience-based and evidence-based knowledge (110). NPMP is a flexible approach focusing on tuning in to meet the different patients’ needs. Hence the approach is difficult to standardize and to find measurements grasping the important changes experienced from the patients’ perspectives, as described above. This might be explanations for why there are few quantitative studies evaluating outcome of the treatment approach.
This scoping review identified 93 studies spanned the years 1975 to 2021. Given the 46- year publication span, the number of studies might look sparce. However, the history, development, and academic positioning of the NPMP approach must then be taken into consideration. First, the treatment approach is developed and established in Norway (3). Secondly, the approach was organized to a specialisation within physiotherapy. Consequently, a limited group of physiotherapists are specialists in the approach. Finally, there are few specialists with an academic competence. The education has recently reached the level of clinical master at three Universities. Over time this might have a significant influence on further research in the field which in turn might further develop the treatment approach.
Research gap and further direction
This scoping review revealed that more research is generally required. There is, however, a gap in the following fields:
· None of the included studies included experiences from children and youngsters, and patients in mental health clinics
· None of the studies included gender perspectives
· None of the studies explored negative experiences from the treatment
· Few studies included immigrant and refugees
· Few studies explored preventive perspectives
· Few studies explored professional education and development
· Few studies evaluated the outcome of the treatment
Strengths and Limitations
To our knowledge, this is the first study identifying the breadth of literature in the field of NPMP. A rigorous methodological approach has been applied and results are presented systematically to give a transparent review of the literature. Since the research in the field is limited with a long publication span, especially the quality of the oldest literature might vary. However, we found it important to include all the chosen studies to get a good picture of the state of the art.
Conclusion
This scoping review examined a total of 93 studies to map the current state of the research in the field of NPMP treatment. The number of studies is limited but has slowly expanded during the last 20 years. Research gap are revealed concerning children and youngsters, men, immigrants, refugees, and patients in mental health clinics. However, research exploring negative experiences from the treatment, preventive perspectives of the approach as well as examination of the professional education and development are also needed.
References
1. WHO. Musculoskeletal conditions. Key facts 2019 [Available from:https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions
2. Bunkan, B.H. [Psychomotor physiotherapy—principles and guidelines]. Tidsskrift for Den Norske Laegeforening. 2001;121(24):2845-8.
3. Thornquist, E. & Bunkan, B.H. What is psychomotor physiotherapy. Oslo: Norwegian University Press. 1990.
4. Grant, M.J., Booth, A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health information & libraries journal. 2009;26(2):91-108. https://doi.org/10.1111/j.1471-1842.2009.00848.x
5. Levac, D., Colquhoun, H., O’Brien, K.K. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69. https://doi.org/10.1186/1748-5908-5-69
6. Arksey, H. & O’Malley, L. Scoping studies: towards a methodological framework. International journal of social research methodology. 2005;8(1):19-32. https://doi.org/10.1080/1364557032000119616
7. Khalil, H., Peters, M., Godfrey, C.M., McInerney, P., Soares, C.B., Parker, D. An evidence‐based approach to scoping reviews. Worldviews on Evidence‐Based Nursing. 2016;13(2):118-23. https://doi.org/10.1111/wvn.12144
8. Sundsvold, M. Muscular Tension and Psychopathology A Comparison of Four Psychopathological Groups by General Physiotherapeutic Examination of Muscular Tension. Psychotherapy and Psychosomatics 1975(26): 219-28. https://doi.org/10.1159/000286933
9. Sundsvold, M., Vaglum, P., Østberg, B. Movement, lumbar and temporomandibular pain and psychopathology. Psychotherapy and Psychosomatics. 1981(35):1-8. https://doi.org/10.1159/000287473
10. Friis, S., Bunkan, B.H., Ljunggren, A.E. What are the basic dimensions of body posture? An empirical evaluation of the Comprehensive Body Examination. I. Nordic Journal of Psychiatry,1998 52(4), 319-326, DOI: 10.1080/08039489850149769
11. Bunkan, B.H., Opjordsmoen, S., Moen, O., Ljunggren, A.E., Friis, S. What are the basic dimensions of respiration? A psychometric evaluation of The Comprehensive Body Examination. II. Nordic Journal of Psychiatry. 1999;53(5):361-9. https://doi.org/10.1080/08039489850149769
12. Bunkan, B.H., Ljunggren, A.E., Opjordsmoen, S. What are the basic dimensions of movements? A psychometric evaluation of the Comprehensive Body Examination III. Nordic Journal of Psychiatry, 2001;55(1), 33-40. https://doi.org/10.1080/080394801750093706
13. Kvåle, A., Ellertsen, B., Skouen, J.S. Relationships between physical findings (GPE-78) and psychological profiles (MMPI-2) in patients with long-lasting musculoskeletal pain. Nordic Journal of Psychiatry. 2001;55(3); 177-184. https://doi.org/10.1080/08039480152036056
14. Kvåle, A., Johnsen, T.B., Ljunggren, A.E. Examination of respiration in patients with long-lasting musculoskeletal pain: reliability and validity. Advances in Physiotherapy. 2002; 4:4; 169-181, https://doi.org/10.1080/14038190260501613.
15. Friis, S., Bunkan, B.H., Opjordsmoen, S. The Comprehensive Body Examination (CBE): From global impressions to specific sub-scales. Advances in Physiotherapy. 2002;4(4); 169-181, https://doi.org/10.1080/14038190260501613.
16. Bunkan, B.H,. Moen, O., Opjordsmoen, S. Interrater reliability of the comprehensive body examination. Theory and Practice. 2002;18(3), 121-129, https://doi.org/10.1080/09593980290058508.
17. Bunkan, B.H., Opjordsmoen, S., Moen, O. Palpation of skeletal muscles: A psychometric evaluation of the muscular items of the Comprehensive Body Examination. Journal of Musculoskeletal pain 2003;11(1) 21-30. https://doi.org/10.1300/J094v11n01_05
18. Kvåle, A., Skouen, J.S., Ljunggren, A.E. Discriminative validity of the Global Physiotherapy Examination-52 in patients with long-lasting musculoskeletal pain versus healthy persons. Journal of Musculoskeletal Pain. 2003;11(3):23-35. https://doi.org/10.1300/J094v11n03_04
19. Kvåle, A., Ljunggren, A.E., Johnsen T.B. Examination of movement in patients with long‐lasting musculoskeletal pain: reliability and validity. Physiotherapy Research International. 2003;8(1):36-52. https://doi.org/10.1002/pri.270
20. Kvåle, A., Ljunggren, A.E., Johnsen, T.B. Palpation of muscle and skin. Is this a reliable and valid procedure in assessment of patients with long-lasting musculoskeletal pain? Advances in Physiotherapy. 2003; 5(3), 122-136, https://doi.org/10.1080/14038190310016526
21. Meurle-Hallberg, K., Armelius, B.Å., von Koch, L. Body patterns in patients with psychosomatic, musculoskeletal and schizophrenic disorders: Psychometric properties and clinical relevance of resource oriented body examination (ROBE-II). Advances in Physiotherapy. 2004;6(3):130-42. https://doi.org/10.1080/14038190310017381
22. Kvåle, A., Skouen, J.S., Ljunggren, A.L. Sensitivity to Change and Responsiveness of the Global Physiotherapy Examination (GPE-52) in Patients With Long-Lasting Musculoskeletal Pain. Physical Therapy. 2005;85(8):712-26. https://doi.org/10.1093/ptj/85.8.712
23. Kåle, A., Bunkan, B.H., Ljunggren, A.E., Opjordsmoen, S., Friis, S. Comparison of two examination methods from Norwegian psychomotor physiotherapy: GPE-52 and CBE. Fysioterapeuten. 2010;77(2):24-32.
24. Kvale, A., Bunkan, B.H., Opjordsmoen, S., Ljunggren, A.E., Friis S. Development of the Posture domain in the Global Body Examination (GBE). Advances in Physiotherapy. 2010;12(3):157-65. https://doi.org/10.3109/14038196.2010.489618
25. Kvåle, A., Bunkan, B.H., Opjordsmoen, S., Friis, S. Development of the movement domain in The global body examination. Physiother Theory Pract. 2012;1(8) 146-154. https://doi.org/10.3109/14038196.2012.704943
26. Friis, S., Kvåle, A., Opjordsmoen, S., Bunkan, B.H. The Global Body Examination (GBE). A useful instrument for evaluation of respiration. Advances in Physiotherapy. 2012;14(4):146-54. https://doi.org/10.3109/14038196.2012.704943
27. Kvåle, A., Bunkan, B.H., Opjordsmoen, S. Development of the palpation domain for muscle and skin in the Global Body Examination. Journal of Musculoskeletal Pain. 2013; 21(1);9-18. https://doi.org/10.3109/10582452.2012.762821
28. Kvåle, A., Bunkan, B.H., Opjordsmoen, S. The Global Body Examination (GBE): A useful instrument for examination of patients with long-lasting musculoskeletal and/or psychological disorders. European journal of Physiotherapy.2016; 18:2, 137-143. https://doi.org/10.3109/21679169.2016.1149217
29. Dragesund, T., Ljunggren, A.E., Kvåle, A. Body Awareness Rating Questionnaire–Development of a self-administered questionnaire for patients with long-lasting musculoskeletal and psychosomatic disorders. Advances in Physiotherapy. 2010; 12(2), 87–94. https://doi.org/10.3109/14038191003706545
30. Dragesund, T., Råheim, M., Strand, L.I. Body awareness rating questionnaire: measurement properties. Physiotherapy Theory and Practice. 2012;28(7):515-28. https://doi.org/10.3109/09593985.2011.642068
31. Dragesund, T., Strand, L.I., Grotle, M. The Revised Body Awareness Rating Questionnaire: Development Into a Unidimensional Scale Using Rasch Analysis. Physical Therapy. 2018;98(2):122. https://doi.org/10.1093/ptj/pzx111
32. Aabakken, L., Aabakken, B., Ofsti, L. Psychomotor physical therapy—patients’ starting point and their evaluation of the therapeutic results. Tidsskrift for den Legeforening.1991;111(13), 1619-1623.
33. Breitve, M.H., Hynninen, M.J., Kvåle, A. The effect of psychomotor physical therapy on subjective health complaints and psychological symptoms. Physiotherapy research International.2010;15(4),212-21 . https://doi.org/10.1002/pri.462
34. Anderson, B., Strand, L.I., Råheim, M. The effect of long-term body awareness training succeeding a multimodal cognitive behaviour program for patients with widespread pain. Journal of Musculoskeletal Pain. 2007;3 (15):19–29. https://doi.org/10.1300/J094v15n03_04
35. Bergland, A., Olsen, C.F., Ekerholt, K. The effect of psychomotor physical therapy on health-related quality of life, pain, coping, self-esteem, and social support. Physiotherapy research international. 2018;23(4):12. https://doi.org/10.1002/pri.1723
36. Dragesund, T., Nilsen, R.M., Kvåle, A. Norwegian Psychomotor Physiotherapy versus Cognitive Patient Education and active physiotherapy—A randomized controlled trial. Physiotherapy Research International. 2021;26(2):e1891. https://doi.org/10.1002/pri.1891
37. Mølstad, E., Barth, K., Nielsen, G.H., Haver, B., Rogge, H., Skåtun, M. A sound soul in a sound body? Changes in muscular and respiratory characteristics after short term dynamic psychotherapy. Tidsskrift for Norsk psykologforening 1995;2(10):220-31.
38. Helöe, B., Heiberg, N.A., Helöe, B., Heiberg, N.A.,Krogstad, B.S. A multiprofessional study of patients with myofascial pain-dysfunction syndrom 1. Acta Odontologia Scandinavica. 1980; 28(2):109-117. https://doi.org/10.3109/00016358009003487
39. Gyllensten, A.L. Psychomotor functioning in suicide attempters ; an explorative study using the Resource oriented body examination of Bunkan. Nordic journal of psychiatry. 1997;51:193-200. https://doi.org/10.3109/08039489709109094
40. Monsen, K., Havik, O.E. Psychological functioning and bodily conditions in patients with pain disorder associated with psychological factors. British Journal of medical psychology. 2001;74(2):183-95. https://doi.org/10.1348/000711201160902
41. Thörnborg ,U., Nordholm, L., Wallström, Å., Svantesson, U. Quality of life assessment for patients with eating disorders. Eating weight disorder. 2005;10:56-60. https://doi.org/10.1007/BF03327551
42. Østerås, N. & Ljunggren, A.E. Muscle pain, physical activity, self-efficacy and relaxation ability in adolescents. Advances in Physiotherapy. 2006; 8: 33-40. https://doi.org/10.1080/14038190600565093
43. Meurle-Hallberg, K. & Armelius, K. Associations between physical and psychological problems in a group of patients with stress-related behavior and somatoform disorders. Physiotherapy Theory and Practice. 2006; 22(1): 17-31. https://doi.org/10.1080/09593980500422354
44. Starrin, L.S. & Klässbo, M. GFM-52 och symtom hos unga kvinnor med huvudvärk och friska. Fysioterapeuten.2007;4: 1.7-23.
45. Kvåle, A., Wilhelmsen, K., Fiske, H.A. Physical findings in patients with dizziness undergoing a group exercise programme. Physiotherapy Research International. 2008;13(3):162-75. https://doi.org/10.1002/pri.402
46. Alstad, E., Stiles, T.C., Fladmark, A.M. Pain reduction by the use of psychomotor physiotherapy? A prospective single-group study. Fysioterapeuten. 2011;78(5):24-32.
47. Wilhelmsen, K. & Kvåle, A. Examination and treatment of patients with unilateral vestibular damage, with focus on the musculoskeletal system: a case series. Physical therapy. 2014; 94(7): 1024–33. https://doi.org/10.2522/ptj.20130070
48 Ask, T, Skouen, JS, Assmus, J, Kvåle, A. Self-Reported and Tested Function in Health Care Workers with Musculoskeletal Disorders on Full, Partial or Not on Sick Leave. Journal of Occupational Rehabilitation. 2015;25(3):506-17. https://doi.org/10.1007/s10926-014-9557-y
49. Dragesund, T. & Kvale, A. Study protocol for Norwegian Psychomotor Physiotherapy versus Cognitive Patient Education in combination with active individualized physiotherapy in patients with long-lasting musculoskeletal pain - a randomized controlled trial. BMC Musculoskeletal Disorders. 2016;17. https://doi.org/10.1186/s12891-016-1159-8
50. Kulsum, N., Haque, M.A., Yasmeen, T., Singh, P.B. Correlation of Global Body Examination (GBE) and St. George’s Respiratory Questionnaire (SGRQ) in Patients with Chronic Obstructive Pulmonary Disorder (COPD).2018: World Journal of Research and Review (WJRR) ISSN:2455-3956, 7:4, 40-48
51. Nøst, T.H., Steinsbekk, A., Bratås, O., Grønning, K. Twelve-month effect of chronic pain self-management intervention delivered in an easily accessible primary healthcare service-a randomised controlled trial. BMC Health Service Research. 2018; 18:1020. https://doi.org/10.1186/s12913-018-3843-x
52. Grønning, K., Nøst, T.H., Rannestad, T., Bratås, O. Participants and developers experiences
with a chronic pain self-management intervention under development: A qualitative study. SAGE Open Medicine. 2018;6:1-9. https://doi.org/10.1177/2050312118817427
53. Hasha,W., Fadnes L.T., Igland, J., Varda,l. R., Giusti, L.M., Stramme, E.M., et al. Two interventions to treat pain disorders and post-traumatic symptoms among Syrian refugees: protocol for a randomized controlled trial.(Report). Trials. 2019;20(1). https://doi.org/10.1186/s13063-019-3919-x
54. Kristiansen, L., Magnussen, L.H., Juul-Kristensen, B., Mæland, S., Nordahl, S.H.G., Hovland, A. Feasibility of integrating vestibular rehabilitation and cognitive behaviour therapy for people with persistent dizziness. Pilot and Feasibility Studies. BMC 2019;5-69. https://doi.org/10.1186/s40814-019-0452-3
55. Knapstad, M.K., Nordahl, S.H.G., Skouen, J.S., Ask, T., Goplen, F.K. Neck pain associated with clinical symptoms in dizzy patients—A cross‐sectional study. Physiotherapy Research International. 2020;25(2):e1815. https://doi.org/10.1002/pri.1815
56. Hasha, W., Igland, J., Fadnes, L.T., Kumar, B., Haj-Youne,S. J., Strømme, E.M. The effect of physiotherapy group intervention in reducing pain disorders and mental health symptoms among syrian refugees: A randomized controlled trial. International journal of environmental research and public health. 2020;17(24):9468. https://doi.org/10.3390/ijerph17249468
57. Buhaug, K., Magerøy, N., Einarsen, S.V., Assmus, J., Kvåle, A. A clinical study of musculoskeletal dysfunction in targets of workplace bullying. European Journal of Physiotherapy. 2021:1-10. https://doi.org/10.1080/21679169.2020.186545
58. Kolnes, L.J., Vollsæter, M., Røksund, O.D., Stensrud, T. Physiotherapy improves symptoms of exercise-induced laryngeal obstruction in young elite athletes: A case series. BMJ Open Sport & Exercise Medicine.2019; doi:10.1136/bmjsem-2018-000487
59. Thornquist, E. Communication: what happens during the first encounter between patient and physiotherapist? Scandinavian journal of primary health care. 1990;8(3):133-8. https://doi.org/10.3109/02813439008994946
60. Thornquist, E. Body communication is a continuous process: the first encounter between patient and physiotherapist. Scandinavian journal of primary health care. 1991;9(3):191-6. https://doi.org/10.3109/02813439109018517
61. Thornquist, E. Varieties of functional assessment in physiotherapy. Scandinavian journal of primary health care. 1994;12(1):44-50. https://doi.org/10.3109/02813439408997056
62. Thornquist, E. Musculoskeletal suffering: diagnosis and a variant view. Sociology of health & illness. 1995;17(2). https://doi.org/10.1111/1467-9566.ep10933380
63. Thornquist, E. Diagnostics in physiotherapy - processes, patterns and perspectives. Part I. Advances in Physiotherapy. 2001;3(4):140-50. https://doi.org/10.1080/140381901317173678
64. Thornquist, E. Diagnostics in physiotherapy á processes, patterns and perspectives. Part II. Advances in Physiotherapy. 2001;3(4):151-62. https://doi.org/10.1080/140381901317173687
65. Nyre, H. & Steinsvik, K. Profesjonell utvikling etter spesialisering i psykomotorisk fysioterapi : kvalitativ intervjustudie. Fysioterapeuten. 2015;7:24-9.
66. Børsum, K. & Råheim, M. Psykomotorisk fysioterapi for pasienter med spiseforstyrrelser. En intervjustudie. Fysioterapeuten. 2017;4(17): 22-8.
67. Løken, H.S & Rise, M.B. Psychomotor physiotherapy for people with adverse childhood experiences – A qualitative in-depth interview study. Fysioterapeuten. 2019;86(8):26-34.
68. Dragesund, T. & Oien, A.M. Demanding treatment processes in Norwegian psychomotor physiotherapy: From the physiotherapists’ perspectives. Physiotherapy Theory and Practice. 2019;35(9):833-42. https://doi.org/10.1080/09593985.2018.1463327
69. Ekerholt, K. & Bergland, A. Learning and knowing bodies: Norwegian psychomotor physiotherapists’ reflections on embodied knowledge. Physiotherapy theory and practice. 2019;35(1): 57-69. https://doi.org/10.1080/09593985.2018.1433256
70. Teigen I., Ekeli, B.V., Sviland, R. «Bruk intuisjonen og fantasien» -ein analyse av kropps- og kunnskapssynet i Aadel Bülow- Hansen si fagutøving og norsk psykomotorisk fysioterapi. Fysioterapeuten; 2020.
71. Ekerholt, K. & Bergland, A. Embodied Knowledge–the Phenomenon of Subjective Health Complaints reflected upon by Norwegian Psychomotor Physiotherapy specialists. Physiotherapy Theory and Practice. 2021:1-12. https://doi.org/10.1080/09593985.2021.1920073
72. Groven, K.S., Ahlsen, B., Dahl-Michelsen, T. Psykomotorisk fysioterapi & covid-19: psykisk helse og samtaler på nye måter. Tidsskrift for psykisk helsearbeid. 2021;18(2):149-61.
73. Forsmo, T. & Holmesland, A.L. License to touch - En intervjustudie om bruk av berøring i behandling av spiseforstyrrelser Fysioterapeuten. 2021;21:56-62.
74. Ekerholt, K. & Bergland, A. The first encounter with Norwegian pyschomotor physiotherapy: Patients’ experiences, a basis for knowledge. Scandinavian journal of public health. 2004;32(6):403-10. https://doi.org/10.1080/14034940410029441
75. Ekerholt, K. & Bergland, A. Massage as interaction and a source of information. Advances in physiotherapy. 2006;8(3):137-44. https://doi.org/10.1080/14038190600836809
75. Øien, A.M, Iversen, S., Stensland, P. Narratives of embodied experiences ; therapy processes in Norwegian psychomotor physiotherapy. Advances in physiotherapy. 2007;9:31-9. https://doi.org/10.1080/14038190601152115
77. Dragesund, T. & Råheim, M. Norwegian psychomotor physiotherapy and patients with chronic pain: patients’ perspective on body awareness. Physiotherapy theory and practice. 2008; 24(4), 243-54. https://doi.org/10.1080/09593980701738400
78. Ekerholt, K. & Bergland, A. Breathing: a sign of life and a unique area for reflection and action. Physical therapy. 2008; 88(7), 832-40. https://doi.org/10.2522/ptj.20070316
79. Ekerholt, K. Awareness of breathing as a way to enhance the sense of coherence: Patients’ experiences in psychomotor physiotherapy. Body, movement and dance in psychotherapy. 2011;6(2):101-15. https://doi.org/10.1080/17432979.2011.568762
80. Sviland, R., Martinsen, K., Råheim, M. To be held and to hold one’s own: narratives of embodied transformation in the treatment of long lasting musculoskeletal problems. Medicine Health Care and Philosophy. 2014;17(4):609-24. https://doi.org/10.1007/s11019-014-9562-0
81. Sviland, R., Martinsen, K., Råheim, M. Towards living within my body and accepting the past: a case study of embodied narrative identity. Medicine Health Care and Philosophy. 2018;21(3):363-74. https://doi.org/10.1007/s11019-017-9809-7
82. Dragesund, T. & Øien, A.M. Transferring patients’s experiences of change from the context of physiotherapy to daily life. International Journal of Qualitative Studies on Health and Well-being. 2020;15(1):1735767. https://doi.org/10.1080/17482631.2020.1735767
83. Dragesund, T & Øien, A.M. Developing self-care in an interdependent therapeutic relationship: patients’ experiences from Norwegian psychomotor physiotherapy. Physiotherapy Theory and Practice. 2021:1-11. https://doi.org/10.1080/09593985.2021.1875524
84. Stokkenes, G. Erkjennelse og anerkjennelse uttrykt som verbal- og nonverbal kommunikasjon mellom pasient og fysioterapeut. Nordisk Fysioterapi. 1999; 3:168-173.
85. Øien, A.M., Råheim, M., Iversen, S., Steihaug, S. Self perception as embodied knowledge-changing processes for patients with chronic pain. Advances in Pphysiotherapy. 2009;11(3):121-9. https://doi.org/10.1080/14038190802315073
86. Øien, A.M., Steihaug, S., Iversen S. Communication as negotiation processes in long‐term physiotherapy: a qualitative study. Scandinavian journal of Caring Sciences. 2011;25(1): 53-61. https://doi.org/10.1111/j.1471-6712.2010.00790.x
87. Sviland, R., Råheim, M., Martinsen, K. Touched in sensation – moved by respiration. Scandinavian Journal of Caring Sciences. 2012;26(4):811-9. https://doi.org/10.1111/j.1471-6712.2012.01024.x
88. Feiberg, M.F. & Thornquist, E. Fysioterapi som relasjonell praksis – behandling af torturoverlevere. Fysioterapeuten. 2016;4(16):16-21.
89. Mølstad, E., Nilsen, G., Barth, K., Haver, B.,Havik, O.E.,Rogge, H., Skåtun, M. Kroppsforhold hos pasienter i psykoterapi. Fysioterapeutens bidra til Bergens-prosjektet om kort tids dynamiks psykoterapi. Tidsskrift for norsk psykologforening. 1989;26:73-9. https://doi.org/10.1080/09593980701738400
90. Sviland, R., Martinsen, K., Råheim, M. If not soma and psyche - what then? Attitude and moveme nt in self development and retention. Fysioterapeuten. 2007;74(12):23-8.
91. Sviland, R., Råheim, M., Martinsen, K. Å komme til seg selv–i bevegelse, sansning og forståelse. Matrix.2009;2:257-275.
92. Sviland, R., Råheim, M., Martinsen, K. Språk–uttrykk for inntrykk.Matrix.2010;2:132-156.
93. Kolnes, L.J. Embodying the body in anorexia nervosa–a physiotherapeutic approach. Journal of bodywork and movement therapies. 2012;16(3):281-8. https://doi.org/10.1016/j.jbmt.2011.12.005
94. Kolnes, L.J. & Stensrud, T. Exercise-induced laryngeal obstruction in athletes: contributory factors and treatment implications. Physiotherapy theory and practice. 2019;35(12): 1170-181. https://doi.org/10.1080/09593985.2018.1474306
95. Øien, A.M. Fortellinger mellom nærhet og avstand til kroppslig erfaring. Fysioterapeuten. 2013;80(3):22-6.
96. Breitve M., Hynninen, M., Kvale, A. Emotional symptoms and health complaints for patients seeking psychomotor physiotherapy. Fysioterapeuten. 2008;75(12):19-26.
97. Ekerholt, K. & Bergland, A. Massage as interaction and a source of information. Advances in physiotherapy. 2006;8:137-44. https://doi.org/10.1080/14038190600836809
98. Solheim, I.J. & Øien, A.M. Rettleiing som kroppsleg erfaring og kritisk refleksjon. Eit Akjsonsforsknings prosjekt. Fontene forskning 2014;1(7):18-30.
99. Øien, A.M. & Solheim, I.J. Supervision of professionals: Interdependency between embodied experiences and professional knowledge. International journal of qualitative studies on …. 2015. https://doi.org/10.3402/qhw.v10.28432
100. Thornquist, E. Face-to-face and hands-on: assumptions and assessments in the physiotherapy clinic. Med Anthropol. 2006;25(1):65-97. https://doi.org/10.1080/01459740500514489
101. Ekerholt, K., Schau, G., Mathismoen, K.M. Body awareness–a vital aspect in mentalization: experiences from concurrent and reciprocal therapies. Phyiotherapy Theory and Practice. 2014; 30(5): 312–18. https://doi.org/10.3109/09593985.2013.876562
102. Kolnes, L.J. Exercise and physical therapy help restore body and self in clients with severe anorexia nervosa. Journal of Bodywork and Movement Therapies. 2017;21(3); 481-94. https://doi.org/10.1016/j.jbmt.2016.09.005
103. Merleau-Ponty, M. Phenomenology of perception.2012. London, Routledge.
104. Øien A.M. Retrospective and emergent narratives of embodied experiences. Fysioterapeuten. 2013;80(3):22-6.
105. Mengshoel, A.M., Sim, J., Ahlsen, B., Madden, S. Diagnostic experience of patients with fibromyalgia–A meta-ethnography. Chronic illness. 2018;14(3):194-211. https://doi.org/10.1177/1742395317718035
106. Werner, A., Malterud, K. It is hard work behaving as a credible patient: encounters between women with chronic pain and their doctors. Social science & medicine. 2003;57(8):1409-19. https://doi.org/10.1016/S0277-9536(02)00520-8
107. Gjengeda,l. E., Sviland, R., Moi, A.L. Patients’ quest for recognition and continuity in health care: time for a new research agenda? Scandinavian Journal of Caring Sciences.2019; 33(4): 978-985. https://doi.org/10.1111/scs.12696
108. Gyllensten, A.L., Gard, G, Salford, E., Ekdahl, C. Interaction between patient and physiotherapist: a qualitative st.udy reflecting the physiotherapist’s perspective. Physiotherapy Research International. 1999;4(2):89-109. https://doi.org/10.1002/pri.156
109. Gard, G. Factors important for good interaction in physiotherapy treatment of persons who have undergone torture: A qualitative study. Physiotheraphy Theory and Practice. 2007;23 (1): 47–55. https://doi.org/10.1080/09593980701209584
110. Skjaerven, L.H., Kristoffersen, K., Gard, G. How can movement quality be promoted in clinical practice? A phenomenological study of physical therapist experts. Physical Therapy. 2010; (10): 1479–92. https://doi.org/10.2522/ptj.20090059
111. Kvåle, A.& Ljunggren, A.E. Body and Mind Therapies. Schmidt R WW, editor. New York: Springer; 2007.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions (https://creativecommons.org/licenses/by-nc/4.0/). Published by Fysioterapeuten.























